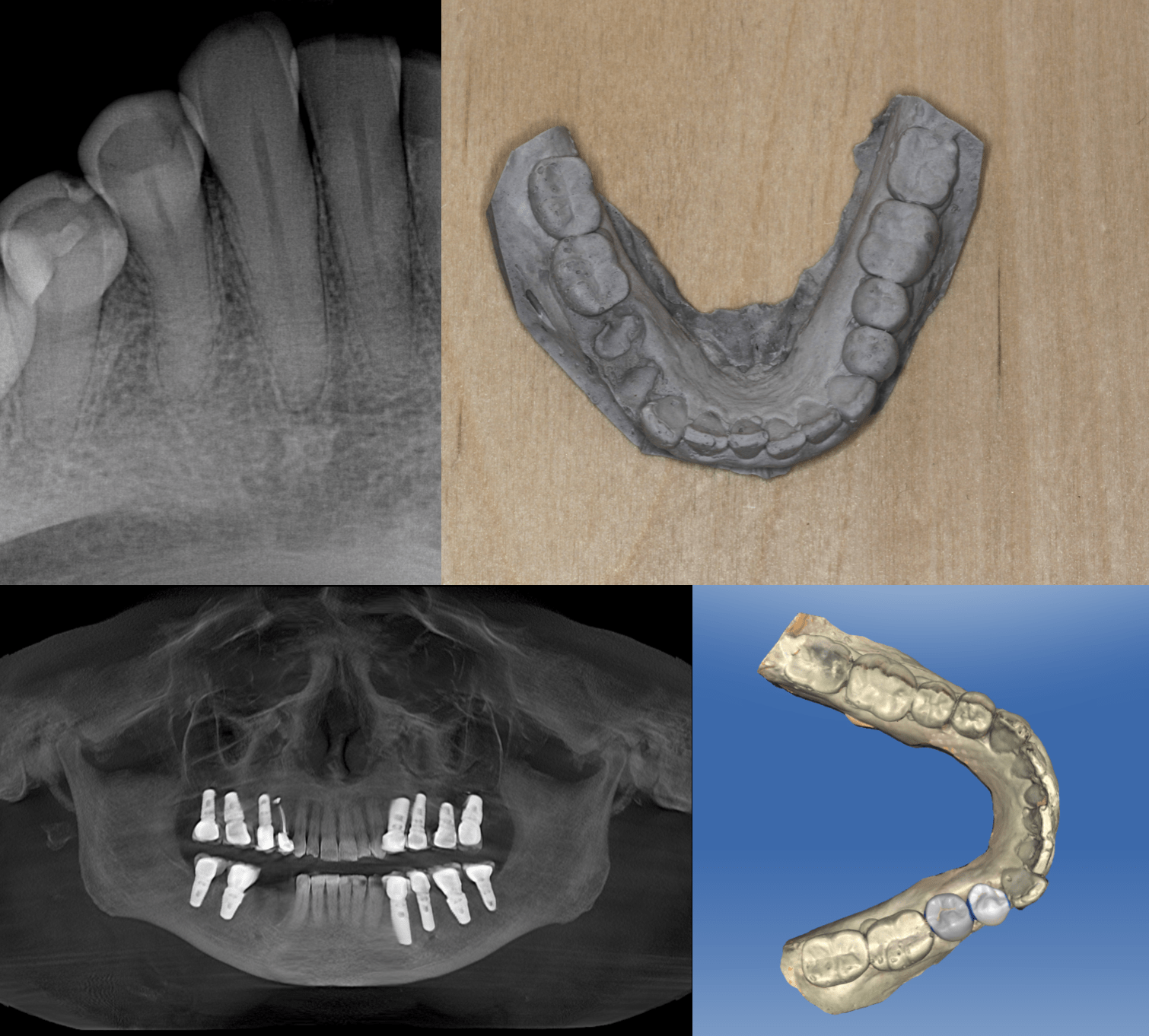
Ok I was really reluctant to post this case as its a little controversial. But what the hell, I’ll post away. This is a great patient that we did a lot of work on over the past 10 years. As you can see we have done a few implants on her. She came in with EXTREME pain on biting, hot and cold on #28 and 29. Some decay on the buccal and some interproximal decay where I would normally just do some crowns and temporize and see if she needed endo. In the past we have done and some endodontists have done RCTs and a few failed. She is convinced that her body “doesn’t like endo.” I know.. weird. So she said she did not want the teeth in there, she is dying and she did not want endo. She stated that my implants feel like normal teeth and she never had pain, so she just wanted to be done and out of pain with #28 and #29. I documented the hell out of it. I know a lot of docs would just tell her to take a hike and not do the implants but knowing her and what a great patient she is and seeing in how much pain she was in, I extracted them. Took an alginate and poured it in fast set stone as the blood was making the Omnicam freak out.
 http://www.Digitalenamel.tv
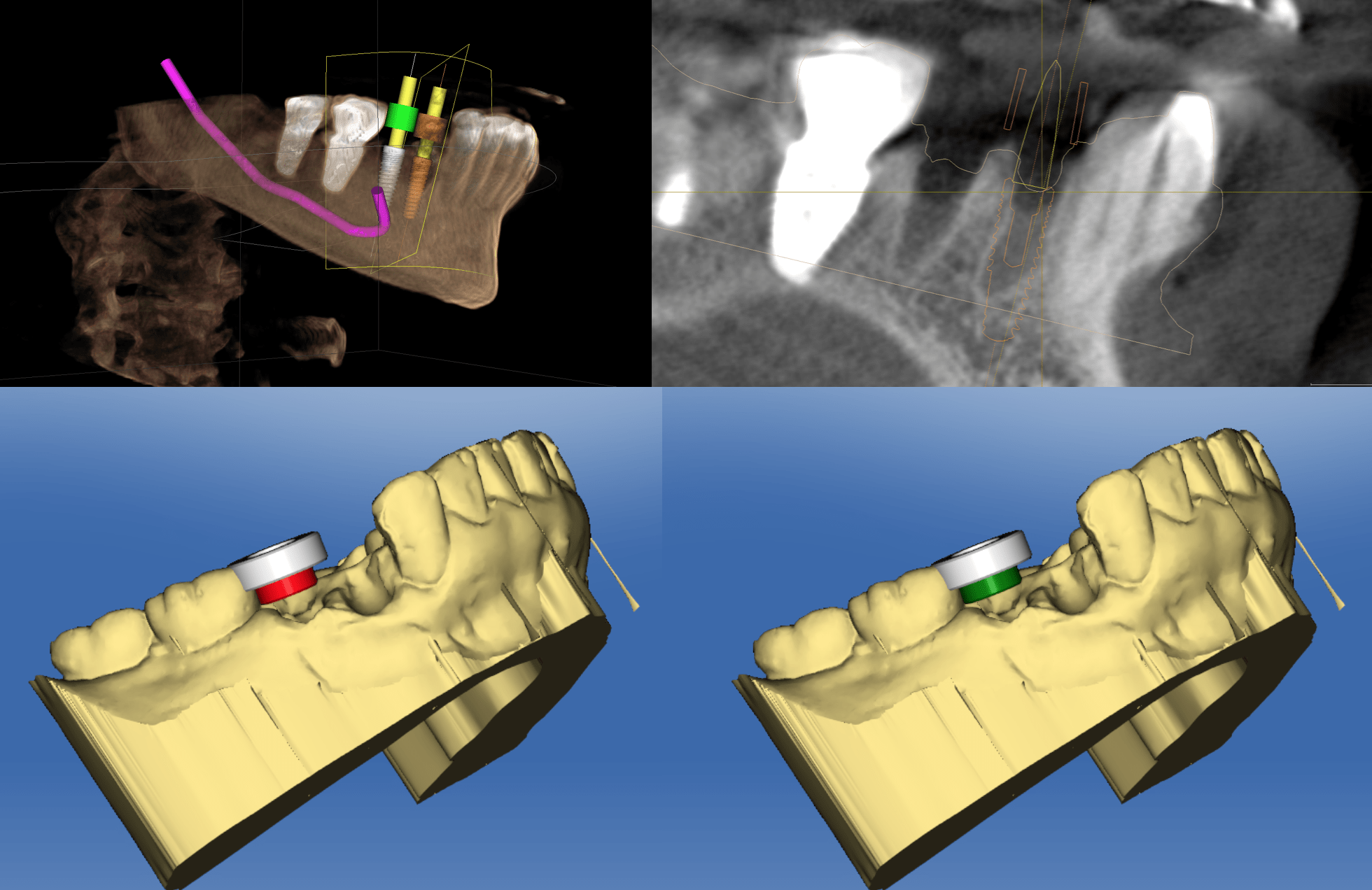
http://www.Digitalenamel.tvAs you may or may not know CEREC guide 2 is a single unit guide so if you want to do two implants you have to make two guides. After taking the alginate and my staff was pouring the model I noticed to get ideal placement I would have to contour #30 to make room. As you can see in the CEREC images we are inside #30 with the sleeve so I opted not to “grind out” that area and took a diamond to the crown on #30.
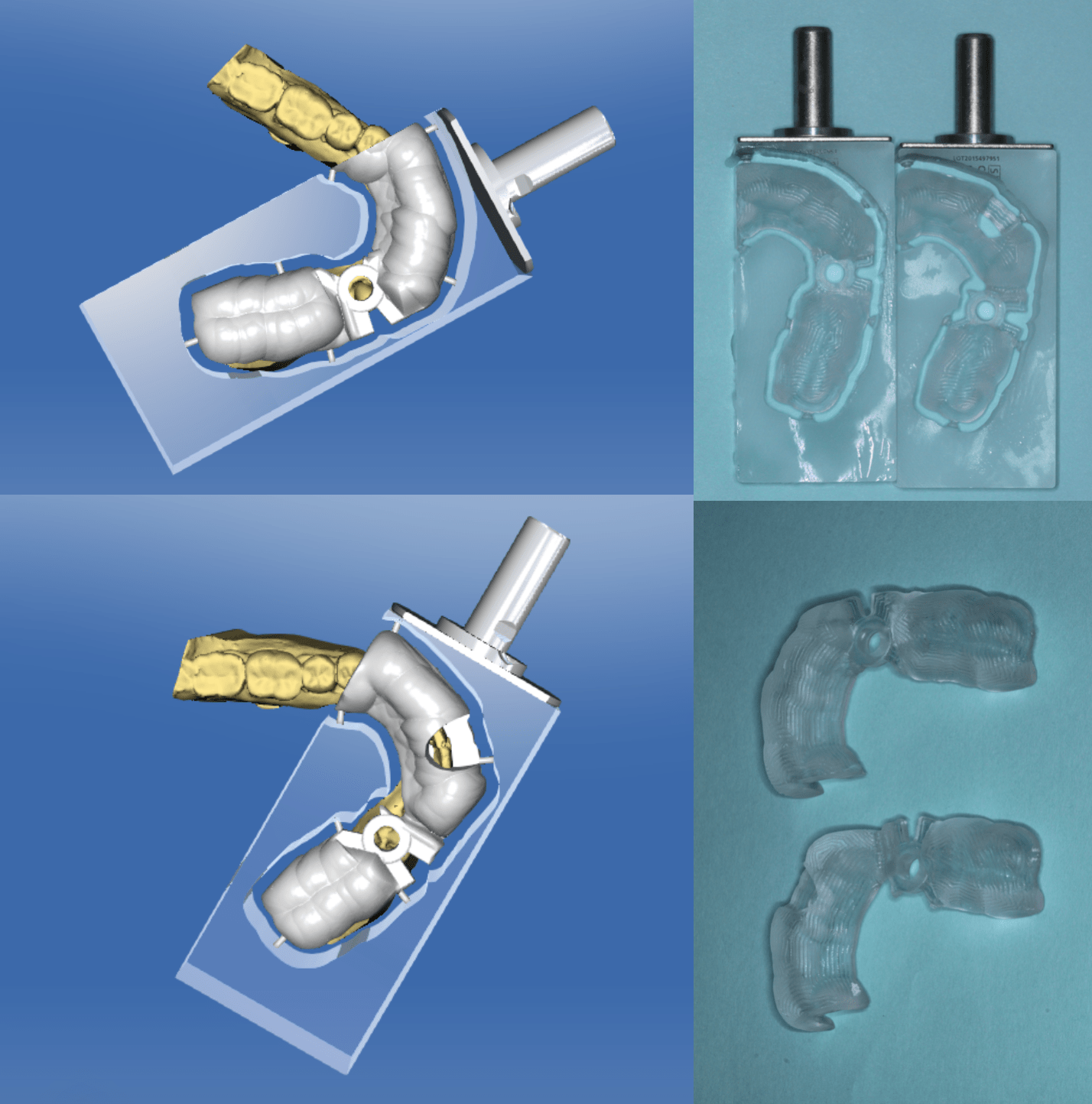
Milled out two guides, with water changing and everything it took about 2 hours but got it done. As you know if a patient wants and immediate implant they really don’t mind waiting so she went to the pharmacy and just chilled in the room while we did this and I saw a few other patients.
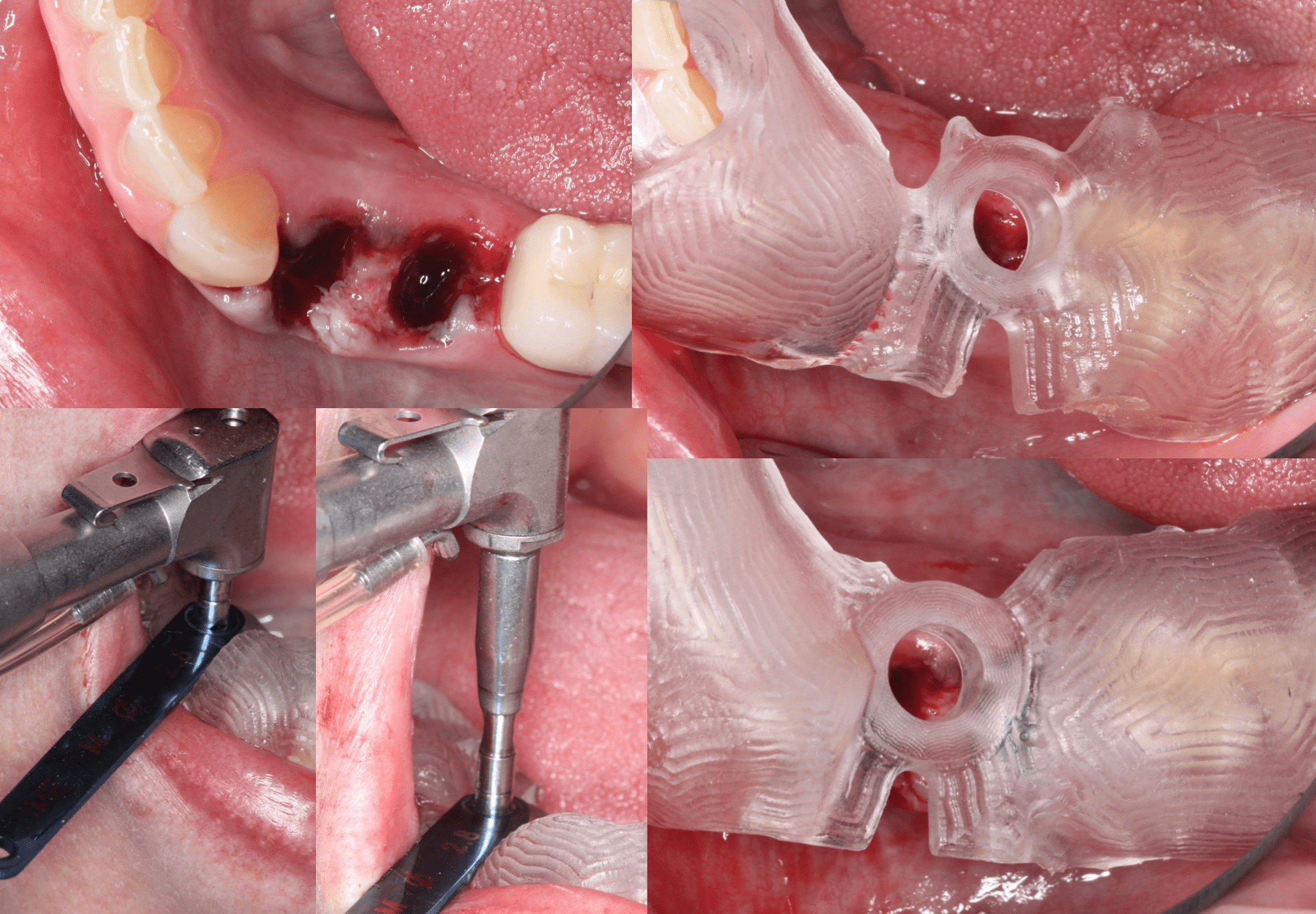
The access for #28 was easy, but since #29 was so close to the crown on #30 I had to use the drill extender to get past. Remember this adds 2mm to your D2. As long as I am not close to any nerves I usually like to drill longer than my osteotomy so I have more control if I need it with stability and platform position. But if I am close to anatomy I stay to my planned length.
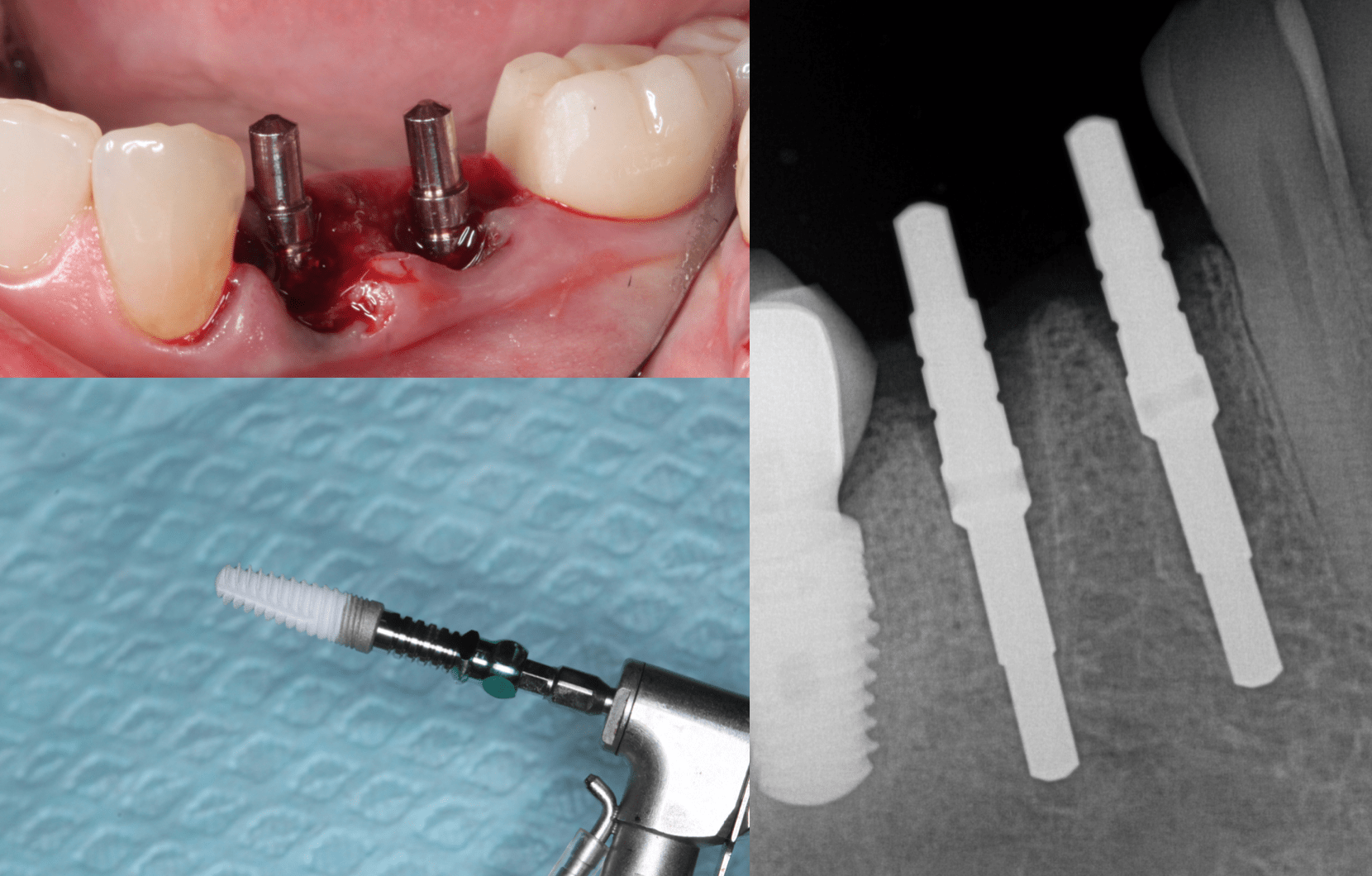
Really smooth surgery. Nice parallel implants. Had a 4.2 by 13 HA legacy 2 and a 4.7 by 13 SBM Legacy 4. Same body just different mounts.
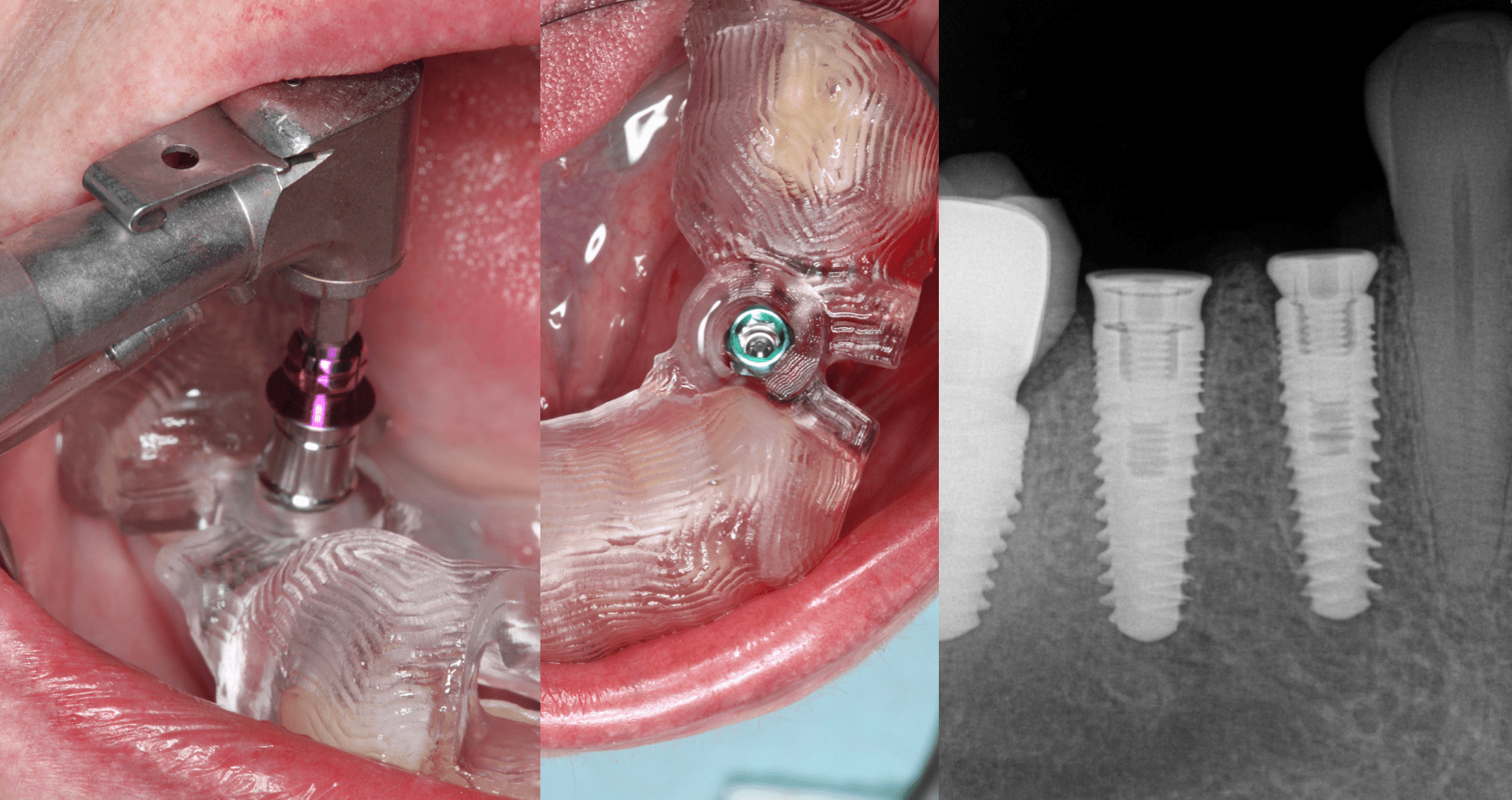
You can easily fit the Legacy 2 through the Medium guide sleeve, but the Legacy 4 mount won’t fit but we got enough implant in so I just removed the mount and placed the freebie healing caps. You can see where I shaped the medial on #30 crown.
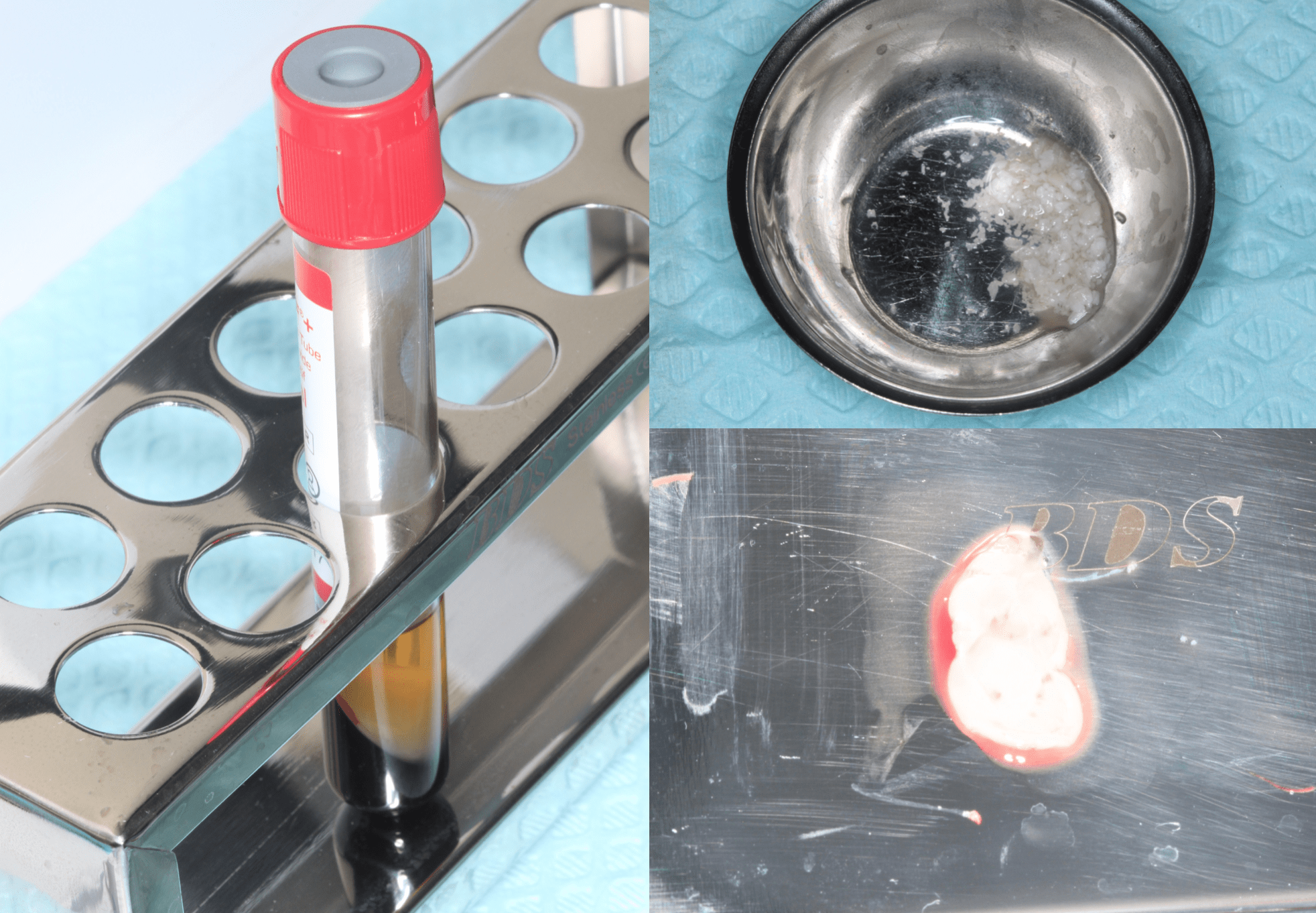
I do PRF when a patient has nice big veins but this patient had nothing so I called one of the nurses next door over. The best she could get was 1/4 of a vial after sticking the patient a ton. So we got what we could and luckily my implant gap distance was not huge. Normally I like 4 vials just so I have enough for the graft and a membrane but we just had enough to mix with graft.
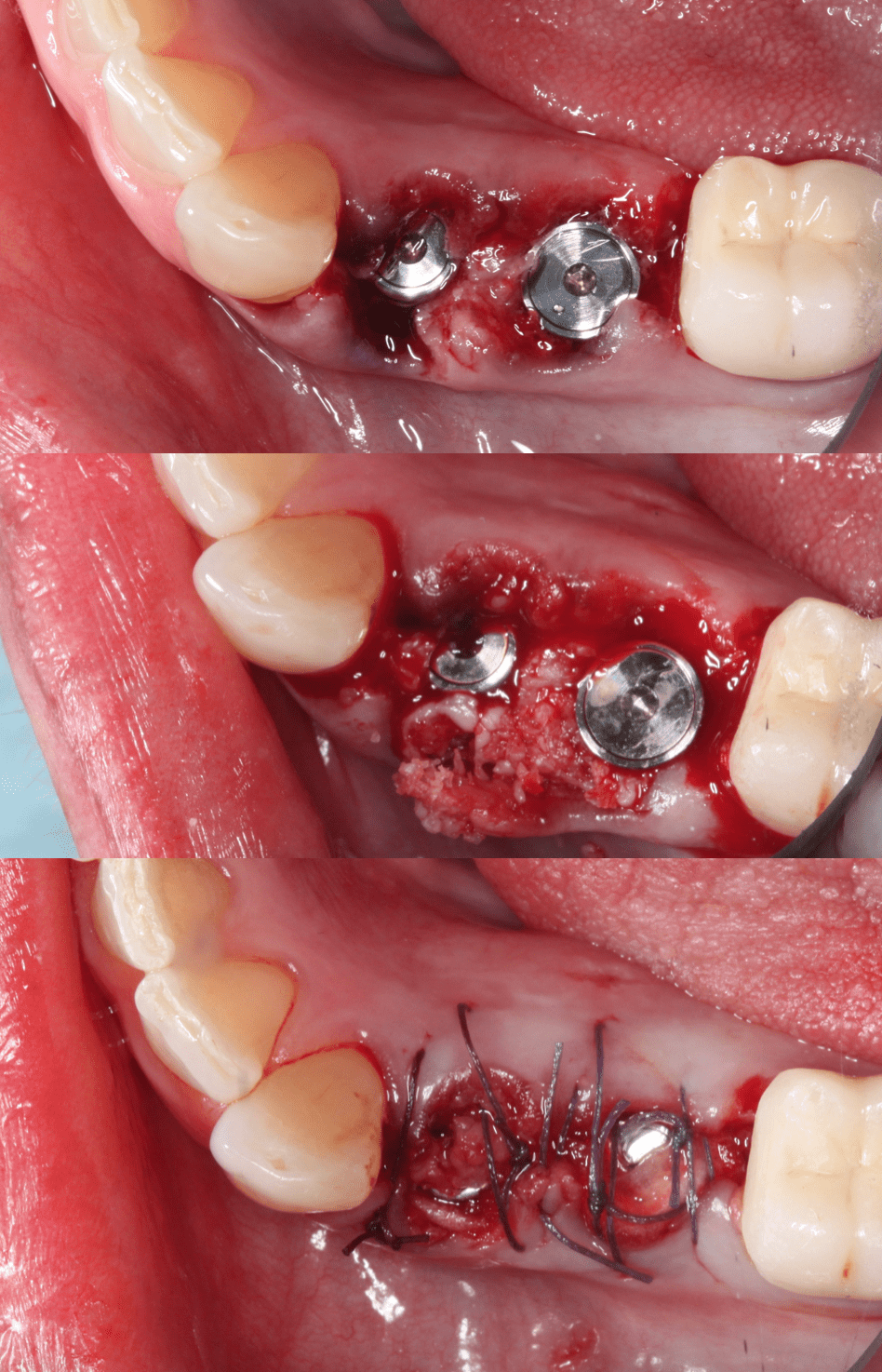
Tucked some shards on membrane on the buccal and sutured up with Villet sutures. Will wait about 6 months to restore. Again, I totally get it if you would not do implants here but the patient was grateful to get out of pain and has always been happy with my implants.
